In this toolkit:

Read this first
Hospitals across the U.S. routinely drug test patients when they give birth, often using urine screens that are easy to misinterpret and have a high rate of false positives. The Marshall Project previously examined how these policies have led to women and families getting reported to child welfare services, investigated and forcibly separated.
In our latest investigation, we discovered that child welfare authorities often forward these reports on to law enforcement. More than 70,000 cases in 21 states were reported to police or prosecutors during a six-year period, according to state and federal data obtained and published for the first time by The Marshall Project.
Many of these women tested positive due to legal CBD products, common foods and medications, and even the fentanyl from their epidurals. As a result, women have been interrogated shortly after childbirth, separated from their newborns, arrested and criminally prosecuted.
To get you started, here is a primer with key takeaways from The Marshall Project’s extensive reporting on drug use investigations for pregnant people. Journalists and researchers are welcome to request a consultation to discuss how to use the resources in this toolkit.
The limitations of hospital drug tests
Hospitals typically use pee-in-a-cup drug tests that are fast and cheap, but they are problematic for several reasons:
-
They are prone to erroneous results, with false positive rates as high as 50%.
-
They are easy to misinterpret because they typically don’t distinguish between illegal and legal substances, so a prescribed medicine could be mistaken for an illicit drug. For example, epidurals often contain morphine or fentanyl and can yield positive results for prescribed opiates, which can then be misinterpreted as an illegal substance.
-
They’re not good at identifying someone with an addiction problem because they don’t show how often or for how long someone may have used drugs.
Some hospitals also test umbilical cords or the baby’s meconium — the first stool. These types of tests also have pitfalls, as hospital-administered medications can be passed on to the baby.
We created the graphic below to shed light on several of the most common foods, household items, and over-the-counter medicines that can cause false positives or test results that can be misinterpreted as illegal substances.
In addition to what’s listed in the graphic, here are other legal drugs and medications that commonly trigger positive tests:
-
Ephedrine and phenylephrine are two different blood pressure medicines often prescribed for C-sections. These can trigger false positives for meth.
-
Vyvanse, a commonly prescribed medicine for ADHD, contains amphetamine, which can be misinterpreted on tests as illegal meth.
-
Many legal CBD and hemp products test positive for THC, marijuana or cannabinoids.
Learn about the data
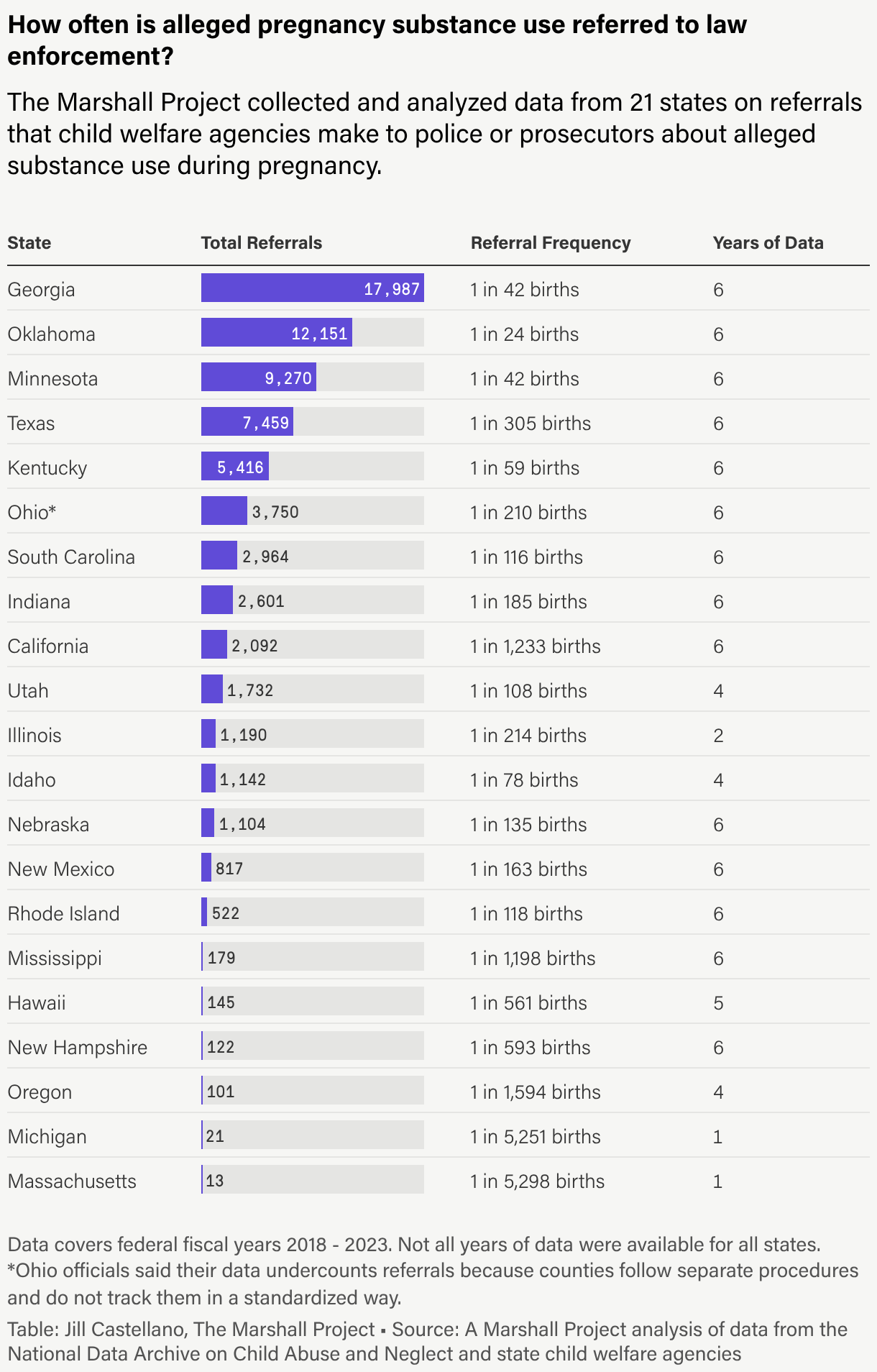
The Marshall Project spent one year compiling and verifying data on law enforcement referrals covering Oct. 1, 2017, through Sept. 30, 2023. Our analysis shows that over that six-year period, child welfare agencies in 21 states referred parents to police or prosecutors more than 70,000 times over alleged substance use during pregnancy. Among those states, Georgia, Oklahoma and Minnesota referred the most cases to law enforcement. Georgia alone referred around 18,000 cases, or one out of every 42 births.
The referral process typically starts when a patient or newborn tests positive for drugs in a hospital. In most states, hospitals are then required to notify child welfare authorities. Even though the drug tests are known to be unreliable, no state requires confirmation testing. State laws and policies dictate whether child welfare must then share those reports with law enforcement. We found that 13 states
State child welfare agencies can voluntarily submit data about alleged pregnancy substance use to the federal Children’s Bureau, which is part of the U.S. Department of Health & Human Services. The records are collected and analyzed by the National Data Archive on Child Abuse and Neglect (NDACAN). While some figures are published in government reports, data on referrals to law enforcement was not publicly available prior to our reporting. The Marshall Project retrieved, verified and analyzed the data from the Children’s Bureau and state child welfare agencies. The data available in each state varies.
To better understand child welfare policies and data in your state, explore the custom data visualization below, designed by data reporters Jill Castellano and Anna Flagg. If you have questions or would like to request a consultation to discuss local coverage, please fill out this form.
In Alabama, the state’s child welfare agency accepted at least 3,403 reports of alleged substance use during pregnancy over six years. It’s unclear how many were referred to law enforcement because the federal program that collects the data did not provide it to The Marshall Project. States are not required to report this information.
Child welfare officials said counties have their own agreements with local police and district attorney’s offices about what child abuse and neglect reports are shared with law enforcement. Referral practices vary across the state.
Limitations of the data
The data we obtained does not cover several important elements of the process for referring parents to law enforcement for suspected substance use:
-
It does not detail what law enforcement did following a referral, such as opening a criminal investigation, arresting or prosecuting a parent or taking no action.
-
It doesn’t provide details on individual cases, nor does it distinguish between cases where police were notified and those where the notification went to prosecutors.
-
It does not specify whether a child welfare investigator determined abuse occurred or if abuse was suspected instead.
-
It doesn’t specify what triggered each report by a medical provider to a child welfare agency.
-
It doesn’t specify why child welfare agencies referred a case — to prompt a law enforcement investigation, to request an officer’s presence if a caseworker feels unsafe or for other reasons.
We also want to flag that because of missing and unverified data, it’s hard to draw some conclusions. For example:
-
With data on law enforcement referrals only available for 21 states, a comprehensive, nationwide analysis is not possible.
-
In eight states,
California, Indiana, Massachusetts, Mississippi, New Hampshire, New Mexico, Oregon, Rhode Island the federal data that The Marshall Project received on law enforcement referrals excluded yearly case counts when they were below 10 cases to protect confidentiality. -
Officials in California, Mississippi and New Hampshire did not confirm the reliability of their data or did not respond to our questions.
You can read more about the data limitations in our methodology.
Background on state child welfare policies
Each state child welfare department follows a set of laws, policies and practices for screening, assessing and referring allegations of pregnancy drug use. The Marshall Project reached out to departments in all 50 states and Washington, D.C., to understand when staff refer these cases to police or prosecutors. This year-long process involved back-and-forth communications with officials to understand the nuances of their work.
Only officials in three states — Louisiana, Mississippi and New Hampshire — did not respond to our questions about their policies. For these states, we relied on statutes and policy documents obtained through public record requests to understand their referral practices.
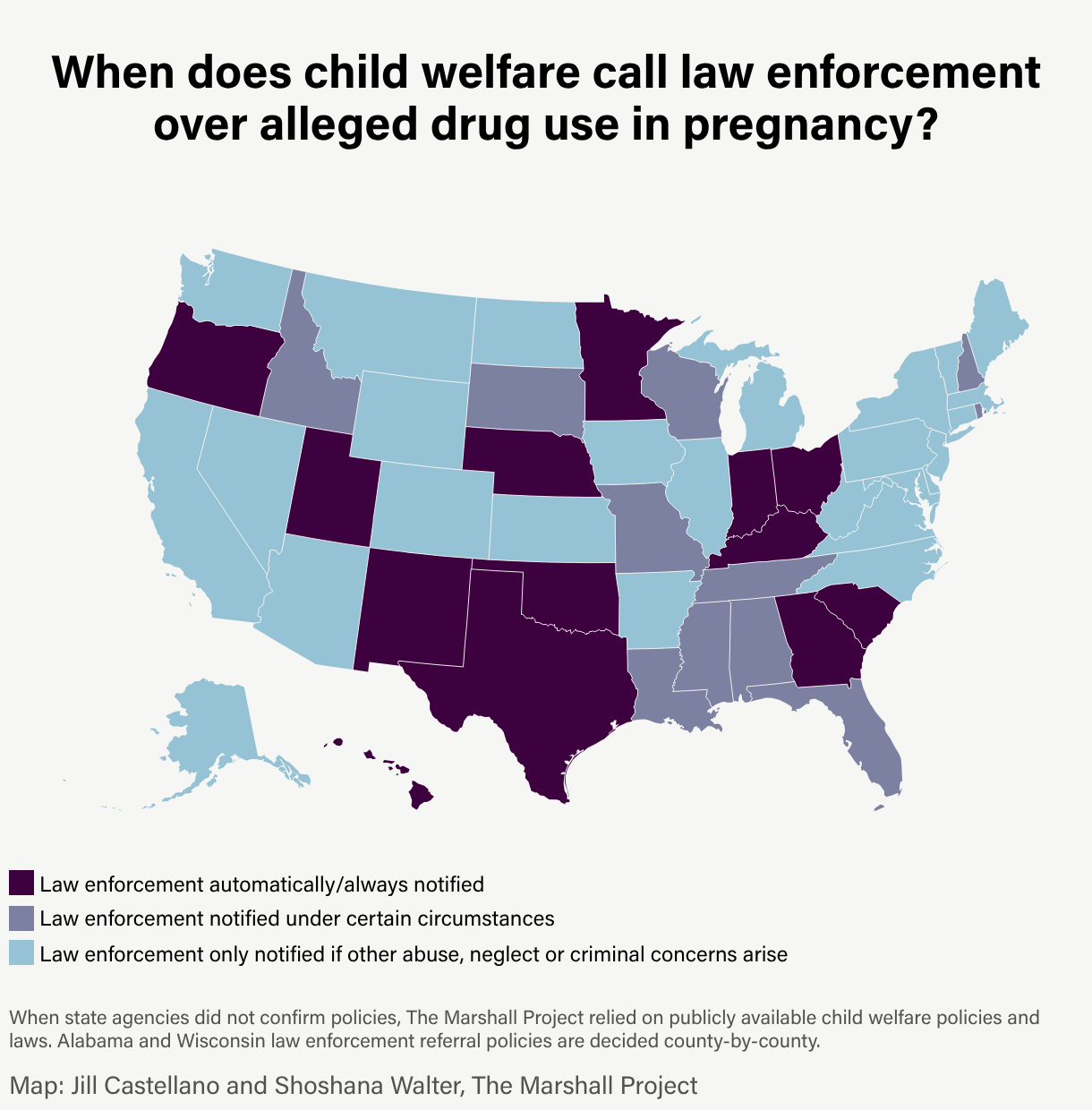
Using all available materials, we classified policies for all states into three categories:
-
Law enforcement automatically/always notified: Child welfare agencies in these states share information with police or prosecutors about all accepted reports of alleged drug use during pregnancy.
-
Law enforcement notified under certain circumstances: An allegation of drug use during pregnancy could prompt a referral in some situations, but not all. For example, referrals may occur only for certain types of illicit substances, or policies may vary by county.
-
Law enforcement only notified if other abuse, neglect or criminal concerns arise: These states do not contact law enforcement if the only concern is drug use during pregnancy. However, the case could be referred if there are other allegations of abuse or evidence of a crime.
We wrote short summaries of states’ policies and gave each state an opportunity to review for accuracy before publication. We adjusted our summaries as necessary based on their feedback.
Access the data
The Marshall Project is making available to the public for the first time the referral data we compiled and summaries of the referral policies for child welfare agencies in all states and Washington, D.C. We encourage anyone using this data to review our methodology, which includes more details on how we acquired, fact-checked and analyzed the data, along with additional findings for several states with high referral rates. You can review the data dictionary here.
You can request a data consultation for your newsroom or classroom here.
State referral policies: For 50 states and Washington, D.C., we provide our written and fact-checked summaries outlining when child welfare agencies refer cases of alleged drug use during pregnancy to police or prosecutors. The file also includes which of the three policy categories we classified each state’s policy into. You can download a CSV file with this information here.
Statistics on state referrals to law enforcement: For each of the 21 states with referral data, we provide state-level statistics on the total number of referrals that child welfare agencies make to law enforcement, the percentage of pregnancy substance use cases that the agencies refer to law enforcement and the number of years of data available. The file also includes our calculation of referral frequency based on the number of live births in each state. You can download it by clicking this link.
Annual data on law enforcement referrals and pregnancy substance use cases per state: The file includes annual breakdowns for the number of allegations of drug use during pregnancy per state that were accepted by child welfare agencies, as well as the number of those allegations that were referred to police or prosecutors. For some states, the data includes how many referred cases involved children deemed victims or nonvictims of child abuse or neglect. We are only publishing fields and years of data that are reliable enough for analysis and that maintain individuals’ privacy. Full or partial data is available for 44 states and Washington, D.C. You can download it here.
Use these free data visualizations
We’ve created two data visualizations that you’re welcome to use. Descriptions of the visualizations and their embed codes are provided below.
The first free data visualization is a national map, distinguishing between states where referrals to law enforcement over alleged substance use during pregnancy always happen, occur under certain circumstances, or only happen if other abuse, neglect or criminal concerns arise. The embed code is provided below and includes all the copy you will need for credits, alt-text, etc. Using the provided embed code should allow you to retain the functionality of hovering over the map on desktop to view policy information for each state. For mobile, users will be able to click on the map.
The second free data visualization is a bar graph, showing the results of our analysis of referral data in 21 states. The most referrals took place in Georgia, Oklahoma and Minnesota. The embed code is provided below and includes all the copy you will need for credits, alt-text, etc.
Note: These assets are also available as still images in various dimensions. If using a still image, make sure to include the provided credit and caption language.
Use this FOIA template
Here is a template to request policies your state child welfare agency follows for screening and assessing substance-exposed newborn reports, and referring such allegations to law enforcement.
Strategies for finding impacted sources
While shedding light on this issue, it’s ideal to include the lived experience of parents who have been impacted by incorrect or misinterpreted drug test results. Here are strategies for connecting with these sources:
-
Scour court records. Child welfare cases are often confidential, but many appellate court rulings are public and available on courtlistener.com. Experiment with search terms, including “positive drug test,” “birth,” “false positive,” “drug screen,” and the names of medications and substances, such as benzodiazepine, methadone, and Suboxone. Tracking recent court filings in your state can help quantify the problem and lead you to attorneys who may have information and sources.
-
Review lawsuits filed by families. Look for cases filed against a hospital or child welfare agency. These suits may be in CourtListener or on the website for your county or district court. Advocates working in this space, such as Pregnancy Justice and your state’s ACLU chapter, may be able to point you to local lawsuits as well.
-
Determine the name of your state’s statute. States have different statutes that they apply to criminal charges for using substances during pregnancy. In Alabama, for example, the charge is called chemical endangerment, while in Idaho, it’s called injury to a child. Go to local prosecutors, law enforcement agencies, and the courts (within towns that have a hospital with a labor and delivery unit) and ask for all case numbers or incident reports filed for that particular charge. This can help you generate a list of people who have been arrested.
-
Search for news clips. You may be able to find the names of people who have been arrested over these allegations by reviewing local news articles or roundups about recent arrests. You can then try reaching out to the family or the person who was arrested to understand what happened beyond what was published. Also, look in the comments section of articles and social media posts about this topic in case impacted people have shared their experiences. You can message those people to find out more.
-
Find support groups. There are many support groups for parents with child welfare cases or children in the foster care system, often on Facebook. Try searching Facebook for child protective or welfare services and the specific agency name in your state. For more sensitive support groups, reach out to the administrator, explaining that you’re a journalist, you would like to join the group to educate yourself, you understand the information is confidential, and you will not publish anything from the page without the permission of the person who posted it. Share links to your staff page and previous related coverage to help verify your identity. Once you’re in a group, you can search its entire history to find posts mentioning specific topics and then reach out directly to those people.
-
Talk to health care providers. There are nurses, doctors, and other health care providers, such as hospital social workers, who have seen parents wrongfully accused of pregnancy drug use. Many of those providers are concerned about this issue. Look for doctors who have done research in this area or who treat patients in labor and delivery or their newborns. Review research in academic journals looking at the impacts of punitive responses to pregnancy drug use and contact relevant authors. If they teach at a university, their contact information may be easier to find.
-
Consider designing a callout to locate sources. Callouts allow you to ask the same set of questions to a wide range of sources at once. As you identify and build relationships with key stakeholders — health care providers, lawyers, caseworkers or support group leaders — you can ask them if they’ll share your callout with their clients or patients. Then, you can follow up with any respondent who fits your story needs. Here is a simple callout we published for this coverage area. Feel free to adapt this language for your local coverage needs (just please credit The Marshall Project somewhere on your callout). And here is a primer on callouts we created for our deaths in custody reporting, which provides important considerations for crowdsourcing reporting.
The Marshall Project has published a callout that is helping our reporters connect with impacted sources. Email us if you’re interested in learning about potential sources in your state.
When incorporating personal experiences of drug use allegations during pregnancy into your reporting, it’s essential to verify every detail to avoid undermining your reporting and your sources. Here are some tips:
-
Tell sources why you must verify every single thing. Along with protecting the validity of your reporting, verifying the facts insulates your sources from unnecessary harm. These folks are uniquely vulnerable to harassment due to the stigma associated with using substances while pregnant. Many women are worried about sharing police and child welfare records with reporters because of how demonizing the allegations may appear. Explain that you need to know everything that has been raised, so you can address all accusations within the reporting. You don’t want to be surprised by an accusation after the story has been published.
-
Be transparent about the reporting process. Let sources know that for the next several weeks or months, you will be requesting access to sensitive records, and you will be asking intrusive questions repeatedly. Explain why this is important, and give your source time to make an informed decision about participating. Check in with them during the reporting process to address any concerns they might have and give them opportunities to ask questions.
-
Ask your source for the results of their hospital drug test and any confirmation test. It’s important to know what kind of drug test the hospital relied upon. Urine screens come with a warning stating that results shouldn’t be used for legal purposes without confirmation testing. Check if the hospital did confirmation testing with mass spectrometry, which offers more definitive results. Some parents may have a confirmation test — which they often pay for themselves — showing they were negative for the illegal substance that appeared in their hospital drug screen. Also, find out what specimen was tested — was it urine, meconium or the umbilical cord? Different types of tests have different pitfalls. Make sure to review your source’s drug test results with a trained toxicologist.
-
Ask for all other related records. Parents may have or be able to obtain medical records confirming medications they were prescribed, along with notes taken by the health care provider and social worker regarding what they reported to child protective services, when they reported it, and details about their interactions with the mother. If the mother was arrested, you can ask for or file a public records request for all police and court records. Before asking sources for their child welfare case records, check state laws to determine if sharing these documents with someone who is not a party to the case is illegal in your state. If so, this risk should be explained to the source before they share any documentation.
-
Be transparent within your reporting. Within the story, explain what facts you were able to verify through official channels and documentation. If you’ve exhausted these approaches and are unable to confirm an allegation, you may need to omit that detail or attribute it solely to the family.
Watch our webinar
The Marshall Project hosted a webinar on April 22, 2026, about various ways that pregnant people are being monitored and policed. Shoshana Walter and Jill Castellano discussed the details of an investigation that uncovered more than 70,000 births in 21 states that triggered referrals to law enforcement over alleged substance use during pregnancy — even though these reports are often based on unreliable hospital drug tests that yield false positive results or are easily misinterpreted.
The event was moderated by Cary Aspinwall, who uncovered how miscarriages and stillbirths are being investigated as crimes in several states. Her reporting shows that how a person handles a pregnancy loss — and where it occurs — can be the difference between a private medical issue and a criminal charge for abuse of a corpse, child neglect or even murder.
Panelists included:
-
Staff Writer Cary Aspinwall is based in Oklahoma and has led a reporting team that documented prosecutions of pregnant people, examined why so many people are serving life without parole sentences and worked on short documentaries with Frontline and our Inside Story team. She has won an Edward R. Murrow Award and a Gerald Loeb Award, and was a finalist for the Pulitzer Prize in local reporting and the National Magazine Awards for public interest.
-
Data Reporter Jill Castellano is based in Los Angeles and covers the uses and misuses of criminal justice data in American society. Before joining The Marshall Project, Castellano worked for ABC television, The Salt Lake Tribune, The Desert Sun and inewsource. She earned a Pulitzer Prize for explanatory reporting in 2018 for her work with USA TODAY on the deaths of undocumented border crossers. While in college at the University of Pennsylvania, Castalleno helped conduct research studies in a criminology laboratory, and she graduated with degrees in criminology and psychology.
-
Staff Writer Shoshana Walter is based in Oakland and is the author of “Rehab: An American Scandal,” from Simon & Schuster. At The Marshall Project, Walter has exposed how hospitals across the country routinely drug test patients who give birth and report them to child welfare authorities based on the results of faulty drug tests. Her reporting has prompted criminal and congressional probes and new laws, and has appeared in The New York Times Magazine, on NPR, on CNN and in newspapers across the country. She has also been honored as a finalist for the Pulitzer Prize and won numerous awards, including the Livingston Award, the IRE Medal and the Murrow Award.
Style and standards
Gender
Match language to what your reporting or data supports. Avoid default gendered language when not supported by reporting; use gender-inclusive language instead. When writing broadly about policies targeting pregnant people — which may include people of multiple genders — use gender-inclusive language:
- pregnant people
- pregnant patients
- patients
- parents
However, when reporting or data specifically refers only to cisgender women, use specific language:
- pregnant women
- mothers
Quote sources and policies accurately, even if gendered. Provide context when relevant.
Substance-related terms
Treat substance use disorders the same way you would report on any other medical condition. When writing about toxicology results, substance use, addiction or recovery, use clinically accurate, non-stigmatizing language. Avoid terms that imply moral judgment, criminality or personal failure.
Default to language that:
- Is medically accurate
- Avoids stigma
- Centers the person, not the condition
- Avoids reinforcing criminal or moral narratives around health conditions
For more guidance on using substance-related terms, refer to the AP Stylebook’s “addiction” entry.
Promote your work
Thank you for using this toolkit to create your own local criminal justice reporting and for other academic and research purposes. Please help us track your work and potentially share it in our newsletter by letting us know what you’ve been working on.
CreditsREPORTING
Shoshana WalterDATA REPORTING
Jill CastellanoDATA EDITING
Aaron Sankin, David EadsEDITORIAL GUIDANCE
Nicole Lewis, Manuel Torres, Ruth BaldwinPROJECT MANAGEMENT
Michelle BillmanMULTIMEDIA GUIDANCE
Marci SuelaDATA VISUALIZATION GUIDANCE
Anna FlaggPHOTOGRAPHY
Andria Lo for The Marshall ProjectVIDEO EDITING
Donald Washington, Jr. PRODUCT
Elan Kiderman Ullendorff, Ana Graciela Méndez, Aithne Feay, Ryan Murphy, Gabe Isman
PRODUCTION GUIDANCE
Mara CorbettAUDIENCE ENGAGEMENT
Ashley Dye, Rachel KincaidSTYLE AND STANDARDS
Ghazala IrshadCOPY EDITING
Ghazala Irshad, Lauren HardieOUTREACH
Terri Troncale, Ruth Baldwin, Michelle Billman